AUCTORES
Globalize your Research

Case Study | DOI: https://doi.org/10.31579/2690-1919/106
Head, Iraq Headquarter of Copernicus Scientists International Panel Baghdad, Iraq.
*Corresponding Author: Aamir Jalal Al Mosawi, Head, Iraq Headquarter of Copernicus Scientists International Panel Baghdad, Iraq.
Citation: Aamir Jalal Al Mosawi. Case Studies in Pediatric Psychiatry: An Approach to Deep Learning and Experience Acquisition. J Clinical Research and Reports, 5(2); DOI:10.31579/2690-1919/106
Copyright: © 2020 Aamir Jalal Al Mosawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 July 2020 | Accepted: 27 July 2020 | Published: 06 August 2020
Keywords: pediatric psychiatry clinic; abnormal behaviors; controlling bowel
It has been disturbingly observed that many learners in the field of medicine, both undergraduate and postgraduate levels may have satisfactory information acquisition in their fields of study, but fail to use it appropriately when it come to clinical practice. One of the important roles of instructors and professional trainers in the field of medicine is to encourage learners to adopt deep learning approaches by making the studied materials interesting and design a curriculum and assessment methods that encourage understanding which help in establishing and creating experience. Deep learning is mostly motivated by the interest in understanding the studied materials and the need to interpret the presented knowledge during the course. Comprehension is the main intention and focus of the learners adopting.
It has been disturbingly observed that many learners in the field of medicine, both undergraduate and postgraduate levels may have satisfactory information acquisition in their fields of study, but fail to use it appropriately when it come to clinical practice. One of the important roles of instructors and professional trainers in the field of medicine is to encourage learners to adopt deep learning approaches by making the studied materials interesting and design a curriculum and assessment methods that encourage understanding which help in establishing and creating experience. Deep learning is mostly motivated by the interest in understanding the studied materials and the need to interpret the presented knowledge during the course. Comprehension is the main intention and focus of the learners adopting deep learning [12, 3].
This special article presents authentic real case studies in child psychiatry aiming at encouraging the learners of this field to adopt deep learning by making these cases interesting with real patients’ photos. These cases which represents major referrals in at the pediatric psychiatry clinic are designed to make comprehension is the essential outcome of learning.
E.K (14 Kg) was born on the second of February, 2012, and was first seen at the pediatric psychiatry clinic at the Children Teaching Hospital of Baghdad Medical city on the 26th of October, 2017. The parents complained that the child was markedly delayed in speaking, had abnormal behaviors, and he was unable to perform daily activities such going to bathroom independently and washes his hands.
The boy was born more than 10 days post-term by caesarean section, and had low birth weight; his birth weight was two kilograms according to the mother. His parents were cousins. His father was a construction worker who was born in 1982. His education was limited to finishing primary school. The mother was a 38-year house wife and her education was also limited to finishing primary school.
The boy was saying only few words and was not saying any two-word sentence. He could say the names of his brother and his two sisters. He didn’t say “Baba” and “Mama” until around the age of two years. The mother thought that the boy was not smiling nor responding to his name during the first year of life, and he was also not looking much to her face. He was also unable to understand simple commands at one year of age. The boy’s motor developmental mile stones were achieved relatively late.
The boy walked holding furniture at around the age of eighteen months. However, when he was seen at about the age of five years and eight months, he could run, and climb stairs normally. He was able to eat independently, but he could not wash his hands nor brush his teeth. He was not controlling bowel and couldn’t go to bathroom independently. However, he was responding to his name, approaches others; engage in games with other children. He could wave goodbye, clap, He also could use non verbal communication (movements) to indicate what he wants, and could imitate others.
The boy was able to understand facial expressions and could make friendship with other children. He had some abnormal behaviors like beating and clinching his mother, hitting things, and threatens to break things when angry. Although he was playing some games on cell phone, he didn’t hold a pencil or scribble. On examination, the child was not cooperative and didn’t respond to any questions and didn’t like taking photo, he tried to escape from the examination room (Figure-1). He didn’t accept taking a pen to scribble or write something.
The boy was treated with research-evidence medical therapies, and the parents were asked to get him a copybook and try to teach him to draw a line, circle, a square.
On the 14th of December the boy was brought to the clinic again.
Although the child was still not that cooperative, he responded to calling his name by turning his head. The mother was happy that treatment enabled her to convince him not to drink much at night and she was thus successful in keeping him dry at night, but he was still not controlling bowel.

Figure-1: The child was not responsive to any questions and didn’t like taking photo and tried to escape from the examination room
The medical treatment enabled the family to teach him many things. They brought his drawings at home including a circle, a square, the sun, a flower, and a face (Figure-2). He was also saying two-word sentences to express some needs. With family help he accepted to write and draw at the clinic. He copied a line, circle, and numbers one, two, four, and five. He was also successful in drawing a man. He also tried to copy his name (Figure-3).

Figure-2: The child’s drawings at home including a circle, a square, the sun, and a face

Figure-3: At the clinic the boy copied a line, circle, and numbers one, two, four, and five. He was also successful in drawing a man. He also tried to copy his name
1-In this case the patient aged five years and eight months, and he was saying only few words including the names of his brother and two sisters. He was not saying any two-word sentence. Which of the following statements is true regarding normal speech development?
A-A normal child says Dada and Mama non-specifically at ten months, and Dada and Mama specifically at one year of age.
B-A normal child says at least six intelligible words at the age of eighteen months.
C-A normal child joins two-three words in sentences at the age of two years.
D-A normal child speaks in sentences and gives full name at the age of three years.
E-All of the above.
2-In this case, the mother thought that her son was not smiling nor responding to his name during the first year of life, and he was also not looking much to her face during infancy. He also was not able to understand simple commands at one year of age. Which of the following statements is true regarding normal personal-social development?
A-A normal infant looks at mother’s face at two weeks of age.
B-A normal infant smiles responsively at 6-8weeks.
C-A normal infant laughs and squeals at four months.
D-A normal infant understand simple commands at twelve months.
E-All of the above.
3-In this case, the mother thought that her son was late in achieving motor development, and she could remember that he walked holding furniture at around the age of eighteen months. Which of the following statements is true regarding normal motor development?
A-A normal child can sit with support at the age of six months.
B-A normal child can sit unsupported for 10 minutes at nine to ten months.
C-A normal child can stand alone for few seconds (1-2 seconds) at one year.
D-A normal child can walk alone at the age of eighteen months.
E-All of the above.
4-Although the patient in this case was delayed in achieving developmental milestones such social smile and walking, the child could run and climb stairs normally. Which of the following statements regarding childhood developmental milestones is true?
A-A normal child can run at two years.
B-A normal child can walk upstairs two feet to a step at two years.
C-A normal child can walk upstairs alternating feet at three years: Walks upstairs one foot per step and downstairs two feet to a step.
D-A normal child can stand on one foot momentarily at three years.
E-A four-year old child can walk-up and down stairs one foot per step with good balances on each foot
F-All of the above.
5-In this case, the boy could eat independently, but he couldn’t wash his hands and brush his teeth. He was not controlling bowel and couldn’t go to bathroom independently. Which of the following statements regarding childhood developmental milestones is true?
A-A one-year old child can drink from a cup.
B-A normal child can drink from cup using two hands at eighteen months.
C-A normal child can use spoon at two years and uses spoon well without much spilling at three years.
D-A two-year old child can indicate need for toilet.
E-A five-year old child can wash and dry face and hands.
F-All of the above.
6-In this case the child could not scribble or draw anything before treatment. Which of the following statements regarding childhood developmental milestones is true?
A-A normal child scribbles at the age of eighteen months.
B-A normal child copies line at the age of two years.
C-A normal child copies a circle at three years.
D-A normal child copies a cross and a square at four years.
E- A normal child copies a triangle at the age of five years.
F-All of the above.
7-The child in this case has:
A-Autism.
B-Attention deficit disorders.
C-Learning disorder.
D-Mental retardation.
E-Non of the above.
8-The boy was treated with new medical therapies which resulted in improving his intellectual abilities and fine motor skills and thus advanced his mental age. The treatments are likely to be:
A-Anti-psychotic drugs.
B-Research evidence based therapies.
C-Methylphenidate.
D-Omega-3.
E-Risperidone.
F-Lamotrigine which inhibits the release of excitatory amino acid neurotransmitters.
9-Which of the following statements about metal retardation is false:
A-It has been called intellectual disability in the DSM-5.
B-The disorder originates during the developmental period before the age of eighteen.
C-It is characterized by significant limitation of cognitive functioning. D-It is characterized by significant impairment of adaptive behaviors which include many of the social and practical skills necessary in everyday life situations.
E-All of the above. F-Non of the above.
10-Patients with mental retardation may have:
A-Attention deficit with difficulties in focusing and remaining focused on a task, and can be easily distracted.
B-Difficulties with language development.
C-Memory impairment including long-term, short-term, and working memory.
D-Poor social development.
E-All of the above.
F-Non of the above.
SJ (Figure-1) was born during the year 2004 by normal vaginal delivery at term following an uneventful pregnancy. She was first seen on the 13th of November, 2017 at the age 13 years. She had alopecia (Figure-1) affecting the eye brows. Her family thought that her intelligence was not that bad, and they tried to enroll her at ordinary primary school, but the school manager refused as she was identified as abnormal.

Figure-1: The patient was first seen on the 13th of November, 2017 at the age of 13 years, and she had alopecia
The girl’s deceased father was born in 1963, and he was graduate of a nursing school. Her mother was born in 1965, she was a house wife, and her education was limited to finishing primary school. She had three sisters and two brothers. Her eldest sister was born in 1983, married and has children, but her education was limited to finishing primary school. Her second sister was born in 1988 and her education was limited to finishing sixth primary school. Her third sister was born in 1991, and her education was limited to finishing third class of intermediate school. Her brothers were born in 1986, and 1990 respectively; the older brother was teacher while the younger brother was studying at college after completing the secondary school. The girl was delayed in achieving developmental milestones: She smiled after the age of sixth months, sat after one year of age, and walked around the age of four. However, when she was seen, she was able to climb stairs, wave goodbye, and clap, eat independently, go to bathroom, wash her hands, and brush her teeth. Her speech was rather good, she can say short sentences, and when asked who am I? , she answered “You are doctor”.
At the clinic, she was cooperative and was happy to take the pen and try to write something (Figure-2). She was as asked to draw a line, a circle, a square, and numbers 1, 2. She copied a line, and a circle, but she couldn’t copy a square. She was able to write only numbers one and two in Arabic (Figure-2).

Figure-2: She was cooperative and was happy to take the pen and try to write something
1-The girl in this case study had all of the followings except:
A-Learning disability.
B-Mental retardation.
C-Autoimmune alopecia.
D-Down syndrome.
E-A generalized neuro-developmental disorder.
F-Non of the above.
2-In this case study, the girl smiled after the age of sixth months, sat after one year of age, and walked around the age of four. Which of the following statements regarding childhood developmental milestones for locomotion is true?
A-Sitting is generally achieved at the age of six months.
B-Crawling is achieved at 9 months.
C-Walking without assistance is achieved at 12-15 months.
D-Running is achieved at 18 months.
E-All of the above.
F-Non of the above.
3-In this case study, the girl was able to copy a line and a circle, but she couldn’t copy a square. Which of the followings is true regarding the order of the development of the ability to copy forms?
A-Copy a line, a circle, a cross, a square.
B-Copy a line, a cross, a circle, a square.
C-Copy a circle, a line, a square, a cross.
D-Copy circle, a line, a cross, a square.
E-The ability to copy certain forms is a fine motor-adaptive skill and develops in a regular order.
F-A and E.
4-When considering to roughly estimating the mental age of the thirteen-year old girl in this case who could copy a circle but not a square by comparing her skills to normal. A normal child who can copy a circle but not a square probably is about:
A-3-4 years old.
B-6-7 years old.
C-8-9 years old.
D-10-12 years old.
5-In this case study, the girl seems to have syndromic mental retardation, which of the following statements is true regarding the types of mental retardation:
A-Syndromic mental retardation is associated with recognizable abnormalities.
B-Patients with non-syndromic mental retardation have no other abnormalities.
C-Down syndrome and fragile X syndrome are common types of syndromic mental retardation.
D-Non-syndromic idiopathic mental retardation accounts for 30 50% of the cases of mental retardation.
E-Genetic causes of mental retardation can be inherited disorders or non inherited disorders associated with mutations in genetic development.
F-All of the above.
6-Which of the following statements is false regarding the causes of mental retardation:
A-Non-syndromic mental retardation can be secondary to brain damage caused by birth asphyxia and meningitis early during life.
B-Preventable causes of mental retardation include congenital hypothyroidism and, phenylketonuria.
C-Trisomy 18 (Edward syndrome) is the most common genetic cause of mental retardation.
D-X-linked mental retardation is a well recognized cause of mental retardation.
E-All of the above.
F-Non of the above.
7-Which of the following statements is true regarding mental retardation:
A-Mental retardation is characterized by significant impairment of intellectual functions, and the IQ score is generally below 70.
B-Mental retardation may present as delays in achieving or failure to achieve milestones in motor skills development such as sitting, crawling, walking.
C-Delayed speech or continued difficulties with speech and language skills after beginning to talk may occur in patients with mental retardation.
D-Behavioral and social problems with difficulties in understanding and following social rules.
E-All of the above.
F-Non of the above.
8-The mental and developmental age of the thirteen-year old girl in this case seems to be less than seven years. A six-year old child is expected to do which of the followings:
A-Draws a person with six parts.
B-Copies diamond.
C-Begins to understand "right" and "left".
D-Identify colors and body parts.
E-All of the above.
F-Non of the above.
9-Mental retardation, in addition to its characteristic association with deficits in cognitive mental functioning, it is also characterized by impairment of adaptive behaviors and adaptive functioning which affect the core activities of daily living and affect everyday general living and include:
A-Skills needed to live independently (or at the minimally acceptable level for age).
B-Daily living skills, such as getting dressed and undressed, using the bathroom, and feeding self.
C-Communication skills, such as understanding what is said and being able to answer.
D-Social skills with peers and family members. E-All of the above.
F-Non of the above.
Y.H was first seen at the age of eight years because of poor language development and abnormal behaviors. The child was born at term by induction of labor, and the mother was having gestational diabetes. The parents were not consanguineous. The father was born in 1966, aged 41 years, and his education was limited to finishing secondary school. The father was a seller working in a shop. The father had non-specific language abnormalities and difficulties. Although, the mother considered the father speech is of not good quality, she was satisfied with his emotional responses. The mother was born in 1970, aged 37, and her education was limited to finishing secondary school.
The boy has three sisters and one brother. The brother was born in 2001 and was studying at third class of intermediate school. His oldest sister was born in 1992 and had very poor progress in school, and she had not finished yet third class of intermediate school. His second sister was born in 1994, and had finished university study of Arabic at the college of arts. The third sister was born in 1997, and was studying at an institute of medical technologies.
The boy’s motor development was considered to be acceptable. He could eat independently, wash hands, dress himself, and go to toilet. In addition, he was able to identify dangers and injurious things like hot objects and fire. However, he smiled late, after three months and babbled at about eighteen months, and was not responding to his name.
The boy’s language was poorly developed. He could say the names of his brother and sisters. He could name some food items like juice, and occasionally was saying short sentences such as “Buy me something”, and “love you dad”. The mother thought that he was looking at her face, with minimal eye contact.
The boy was sometimes able to express desires by making movements, and gestures. He was also infrequently waving goodbye, and claps.
The boy was generally not approach others, nor engaging in group games with other children or share his interests with others. He was not imitating others, and had poor understanding of facial expressions.
He had obvious repetitive behaviors including hand flapping, and head rolling. He sometimes became preoccupied with rotating things like fan and things that he could rotate or move it in a circle such as a rosary.
The mother also reported violent actions like breaking glass of windows when angry, and the most notable aggressive behavior was biting his mother.
On examination, the boy was hyperactive, not responding to calling his name, and it was difficult for the mother to make him sit down (Figure-1).
He had minimal, if any eye contact and was not looking at faces. When he sat on the chair he was not looking at the doctor, and when the mother gave him a pen he didn’t follow the doctor’s request to draw a line or scribble. The mother and his sister convinced him to try to draw a line, but he could only scribble.
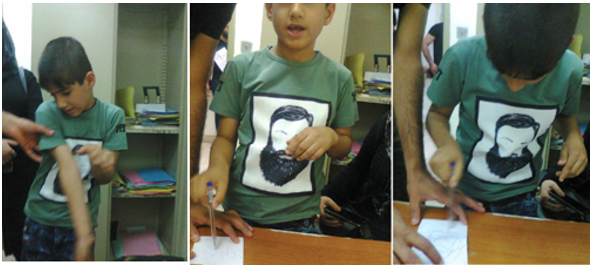
Figure 1: The boy was hyperactive, not responding to calling his name, and it was difficult for the mother to make him sit down
1-Features suggesting typical or classical autism in this case include all of the following except:
A-Poor language development.
B-Looking at his mother’s face with minimal eye contact.
C-The child reluctance to approach others, to engage in group games with other children, and also reluctance to share his interests with others.
D-The boy’s inability to imitate others, and his poor understanding of facial expressions.
E-The repetitive behaviors including hand flapping, and head rolling.
F-His inability to draw a line.
2-Features displayed by this child that are against the diagnosis of autism include:
A-The boy’s acceptable motor development.
B-The boy’s ability to eat independently, washes hands, cloth himself, and go to toilet.
C-The boy’s ability to identify dangers and injurious thinks like hot objects and fire.
D-The boy’s preoccupation with rotating thing like fan and things that he can rotate or move it in a circle such as a rosary.
E-All of the above.
F-Non of the above.
3-Which of the following statements regarding autism is true:A-Symptoms of autism begin slowly after the age of six months, and become established by the age of two or three years.
B-Significant social impairments make autism distinctive from other developmental disorders especially mental retardation.
C-The characteristic symptoms include impairments in communication, and restricted interests and repetitive behavior.
D-The diagnosis of typical and classical autism requires that symptoms become apparent before the age of three years.
E-All of the above.
F-Non of the above.
4-Early features of autism include:
A-Delayed onset of babbling.
B-During infancy patients with autism show less attention to social stimuli, smile and look at others less often.
C- Autistic children show less response to their own name.
D-All of the above.
E-Non of the above.
A.A was born in 2009, and was first seen on the 25th of December, 2017 because the mother was complaining that he had poor social interaction despite she thought that his intellectual function and language development was good.
The boy was born at term by normal vaginal delivery after an uneventful pregnancy, and his birth weight was 2900 grams. The parents were not relatives; the mother was Syrian and the father was Iraqi. The father is a professor of history who was born in 1965, and the mother was born in 1987, and had a university certificate from college of management and economy in Syria. The patient has an older brother aged 9 years who was studying at fourth grade primary school. The boy didn’t experience delay in motor development and language development and babbled during the first year. When he was seen, he could sing a song. His adaptive behavior was satisfactory as he could eat, drink, and go to bathroom, wash hands, change clothes, and brush teeth.
He was playing with his brother, and could identify dangers. He didn’t show aggressive behavior, but he was beating his brother because of jealous. He points to the things he wants, wave goodbye, and clap. The boy displayed repetitive movements mainly in the form of head nodding.
At the clinic, the boy was not that cooperative, and showed minimal eye contact and minimal looking at face. The boy was not responsive to the doctor, but he was more responsive to his mother when she asked him to draw a circle and to write a word (Figure-1), but he started to play with the pen instead of drawing. The boy could draw circle, but the word he wrote was not that good .When his name was called more than one time to bring his attention and asked to look on the O clock on the wall, he looked at the wall (Figure-2).

Figure-1
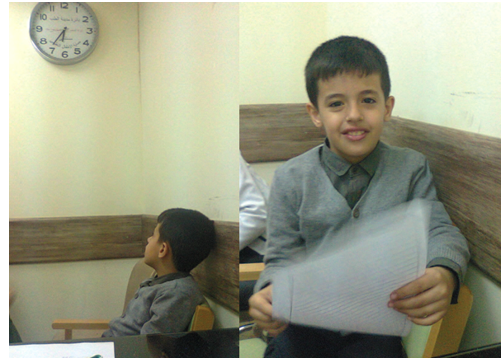
Figure-2: When his name was called more than one time to bring his attention and asked to look on the O clock on the wall, he looked at the wall. The boy was also responsive to his mother when she asked to make a cheese to take a photo and looked at the camera
1-Features in this child that are against or not in favor the diagnosis of classical autism include:
A-The father is professor and the mother has a university certificate.
B-The child normal motor development.
C-The child was babbling during the first year of life.
D-Acceptable language development.
E- C and D.
F-None of the above.
2-Features in this child that are not much in favor of the diagnosis of autism include:
A-The boy’s adaptive behavior was satisfactory as he can eat, drink, go to bathroom, wash hands, change clothes, brush teeth.
B-The boy’s ability to identify dangers.
C-The boy points to the things he wants, wave goodbye, and clap.
E- All of the above.
F-None of the above.
3-The child in this case most likely has:
A-A pervasive developmental disorder.
B-Classical autism.
C-Asperger syndrome.
D-Attention deficit hyperactivity disorder.
E-A and C.
F-Non of the above.
4-Features of Asperger syndrome include all of the followings except:
A-Significant difficulties in social interaction.
B-Difficulties in nonverbal communication.
C-Restricted and repetitive patterns of behavior and interests.
D-Markedly retarded speech development.
E-Manifestations generally start before the age of two years.
F-Non of the above.
5-Which of the following statements is true:
A-Asperger syndrome differs from autism by relatively normal language or better language development.
B-Asperger syndrome as a separate disorder was removed in the 2013 fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), and was included within the autism spectrum disorder.
C-Asperger syndrome is present as a separate disorder in the tenth edition of the International Classification of Diseases (ICD-10) as of 2016.
D-Asperger syndrome is considered by the DSM-5 as a milder autism spectrum disorder.
E-All of the above.
F-Non of the above.
Hadeel was first seen during November, 2017 at the age of four (Weight: 22 Kg) because of non-development of speech, marked hyperactivity and abnormal behaviors. She was born at term by normal vaginal delivery after what considered an uneventful pregnancy. Her parents were relatives. The father was a retired military aged 54 and the mother was a house wife aged 37, and her education was limited to finishing primary school. The girl had an older brother aged thirteen years studying at first intermediate school, and an older sister aged ten who was studying at fourth class primary school. The girl didn’t’ have significant motor delay as she walked at the age of eighteen months. Her speech was not developed and she was not saying any single word. The girl was very late in babbling and was saying only one letter at the age of two years. She was not shown social smile during infancy. She was not looking at faces nor responding to own name. She was not approaching others nor was engaging in games with other children. She was not imitating nor was sharing interest with others. She was not showing any attachment to her siblings or parents nor could she understand their facial expressions. She was not pointing to things to express desire, nor was waving goodbye, but she was clapping very rarely. The girl could help her self with urination only, but she could not wash hands nor brush her teeth. She was displaying some repetitive movements especially hand flapping and head rolling. She was preoccupied with watching cartoons on TV, but she has no special preoccupation with a toy or game. She was biting her clothes and beat her mother and sister.
At the clinic she was very hyperactive and was very difficult to control, she was not interested in taking photos and was obviously reluctant to look at faces. However, she became interested in the soap and tried to eat it (Figure-1).

Figure-1: At the clinic, the girl was very hyperactive and very difficult to control, but she became interested in the soap and tried to eat it
Thereafter, It was possible to have her attention, it was possible to make her interested in a pen and she took the pen. It took some time to make her try to draw a line and a circle. The girl scribbled and could draw a circular figure, but not a circle (Figure-2).

Figure-2: It was possible to have her attention, and it was possible with help of the father to make the girl interested in a pen and she took the pen. It took some time to make the girl try to draw a line and a circle. The girl scribbled and could draw a circular figure, but not a circle
1-Features in this four-year old girl that suggest the diagnosis of autism include:
A-Acceptable progress of motor development.
B-Poorly developed speech without saying any single word at the age of four.
C-Delay in babbling with single letter at the age of two.
D-Lack of social smile during infancy.
E-All of the above.
F-None of the above.
2-All of the following features in this four-year old girl suggest the diagnosis of mental retardation except:
A-Acceptable progress of motor development.
B-Poorly developed speech without saying any single word at the age of four.
C-Delay in babbling with single letter at the age of two.
D-Lack of social smile during infancy.
E-All of the above.
F-Non of the above.
3-Features in this four-year old girl that are more characteristic of autism and in favor of the diagnosis of autism rather than mental retardation include:
A-The girl was not looking at faces nor responding to own name.
B-The girl was not approaching others nor was engaging in games with other children.
C-The girl was neither imitating nor sharing interest with others.
D-The girl had repetitive movements especially hand flapping and head rolling.
E-The girl was not pointing to things to express desire, nor was waving goodbye.
F-All of the above.
4-Features in this four-year old girl that are in favor of the diagnosis of mental retardation rather than autism include:
A-Hyperactivity that made her difficult to control.
B-The child attempt to eat soap.
C-The girl’s preoccupation with watching cartoons on TV.
D-The girl inability to copy a line and a circle.
E-B and D.
5-The girl in this case most likely has:
A-Mental retardation with autistic features.
B-Classical autism.
C-Atypical autism with mental retardation.
D-Attention deficit hyperactivity disorder.
E-A and C.
F-Non of the above.
Mahdi AA was born on the 6th of November, 2014, and was first seen at the pediatric psychiatry clinic of the Children Teaching Hospital of Baghdad Medical City on the 19th of October, 2017, at the age of three years.
The mother complained that the child had abnormal behaviors that started early during the second year of life. The mother considered the boy’s development to be normal during all of the first year of life. He smiled at the age of eight weeks, and had facial preference, and was responding to his name. His verbal language developed normally during the first year of life as he was babbling at the age of nine months, and he was babbling with more than one consonant (B, D) before the end of the first year. The boy’s non-verbal communication was also good as he was pointing to the things he wanted and was waving goodbye during the first year of life. During the first year, he was operated for left inguinal hernia which was diagnosed during the second month of life. The boy’s motor development progressed in an acceptable fashion as he sat at the age of six months, and was walking confidently at eighteen months However, early during the second year; the child began to lose many of the social and communication skills that he acquired during the first year. He became less responsive to his name and was not looking at faces, and he was no longer pointing to things he wants or things of interest. He was also showing abnormal movements such as body rocking, teeth grinding and head banging. The boy’s speech was not progressing anymore, but he developed echolalia. The parents were not relatives. The father was a daily worker, and his education was limited to finishing secondary school. The father was regarded as an isolated boy during childhood as he didn’t play much with other children and didn’t develop significant friendship during childhood. However, the mother thought that the father as an adult has normal social and emotional interactions. The mother was a house wife despite she studied physics at university and received a bachelor degree. The boy had a normal brother aged thirteen who was doing well at first year intermediate school. At the pediatric psychiatry clinic (Figure-1), it was possible to bring his attention initially for short time. However, the boy was hyperactive and showed poor response to name, and he left the room twice. It was necessary to lock the door of the room to keep him inside, but he tried to leave again and in his attempts, he noticed the electric switch of the lights of the room. He was repetitively switching off the lights, and it was difficult to stop him doing this using verbal communication. However, with help of the mother, it was possible to bring his attention again, but he turned his head again to look at the electric switch of the lights of the room, but it was possible to bring his attention to the paper which he caught. The mother convinced him to take the pen and to scribble .He couldn’t draw a circle or even a line. When the doctor was pointing to the O clock on the wall and asked to look at it, he looked at the hand of the doctor instead of the O clock.

Figure-1
1-The boy in this case most likely has:
A-Regressive autism.
B-Classical autism.
C-Attention deficit hyperactivity disorder.
D-A and C.
E-Non of the above.
2-Which of the following statements is true:
A-In the most common form of autism, manifestations are present early in infancy.
B-In a less common form of autism, an initial period of normal development is followed by discontinuation or significant slowing of the acquisition of communication and/or social skills and the patient reaches a developmental plateau.
C-In an uncommon form of autism, a period of normal or near normal early development is followed not only by cessation of normal development, but loss of previously acquired communication and/or social skills also occur.
D-All of the above.
E-Non of the above.
3-Disorders that can be associated with symptoms of regressive autism include:
A-Fragile X syndrome.
B-Tuberous sclerosis.
C-Rett syndrome.
D-Mitochondrial disorders.
E-Landau-Kleffner syndrome (an epileptic encephalopathy).
F-All of the above.
4-Which of the following statements is true:
A-About one third of children with autism and autism related disorders may have regressive autism
B-In contrast to classical autism, patients with regressive autism experience normal early development followed by loss of language and social skills.
C-Research evidence has suggested that regressive autism could be an inflammatory or auto-immune disorder.
D-Research evidence has suggested steroids may have a role in the treatment of regressive autism.
E-All of the above.
F-None of the above.
Maya (Figure-1) was born on the 4th of May, 2013 and was seen on the 11th of December 2017 because her mother thought that despite the girl has normal intelligence, she doesn’t have adequate social interaction manifested mostly by not responding to calling her name normally.

Figure-1
The girl was born at term by cesarean section because of previous cesarean section, and pregnancy was uneventful. Her birth weight was about four kilograms. The parents were not relatives. The father aged thirty two and he was fourth year neurosurgery resident. The mother was thirty-year old, and she was unemployed despite having master in computer science. The girl had one brother doing well at first grade primary school. The girl had normal motor development, she sat at 6 months and walked at one year and now she can run and climb stairs normally. The girl’s adaptive behaviors were normal as she could eat normally, go to bathroom independently, wash hands and brush her teeth. The girl was also able to write her name and can count to ten. She could identify dangers and didn’t display aggressive behavior or self- injury behavior tendency.
The mother didn’t know when her daughter began to smile socially, but she was seen, she was waving goodbye, and like to play with her brother, but she was not seen to clap. The girl didn’t have repetitive or any abnormal movements, but some time she was repeating words. She was not obviously preoccupied with anything.
1-The girl most likely has:
A-Classical autism.
B-Atypical autism.
C-Asperger syndrome.
D-Childhood disintegrative disorder.
E-A and D are possible.
F-Non of the above.
2-Pervasive developmental disorders include:
A-Autism.
B-Asperger syndrome.
C-Childhood disintegrative disorder.
D-Rett syndrome.
E-Pervasive developmental disorder not otherwise specified (PDD-NOS).
F-All of the above.
Ashraf (Figure1) was born during June, 2008 and was first seen at the pediatric psychiatric clinic of the Children Teaching Hospital of Baghdad Medical City at the age of ten during April, 2018. The parents were unrelated.

Figure-1
The father was a forty-year old porter, and his education was limited to finishing fifth grade of primary school. The mother aged thirty years, and her education was limited to finishing third grade of intermediate school. The boy had an older sister aged fifteen years and an older brother aged thirteen, they were studying at third grade and first grade of intermediate school respectively.
The boy was studying at fourth grade primary school and his school performance was considered acceptable. However, the child was brought to our clinic because they were saying in school that the boy is crazy because of abnormal behaviors.
The boy abnormal behaviors included:
Shrugging his shoulders
Shrugging his hips with unusual movements of the legs as if he was dancing.
Unusual facial grimace and lip licking.
Licking the back of his hand.
Producing abnormal sounds from his throat.
The parents were reproaching the boy and asking him to stop doing these behaviors, but in vain. The child was obviously embarrassed from these behaviors and was trying to avoid talking about them, but he confirmed that he can not stop them. The boy had been experiencing these abnormal behaviors for more than one year.
At the clinic the child was cooperative and responding, but he was obviously trying to avoid talking about his abnormal behaviors because of embarrassment.
1-The child most likely has:
A-Childhood schizophrenia.
B-Psychotic reaction.
C-Rheumatic chorea.
D-Huntington chorea.
E-Non of the above.
2-The boy received a medication and when seen after one week, he had obvious amelioration of his disorder. The most likely medication received is:
A-Baclofen.
B- Orphenadrine.
C-Haloperidol.
D-A phenothiazine.
E-Non of the above.
3-Which of the following statements is false:
A-Tics are involuntary, repetitive, non-rhythmic movements that may affect any muscle group, and are commonly intensified by stress.
B-Tics disorders include transient tics of childhood, chronic tics disorder, and Gilles de la Tourette syndrome.
C-Gilles de la Tourette syndrome is the most common movement abnormality of childhood.
D-All of the above.
E-Non of the above.
4-Which of the following statements is false:
A-Tics are commoner in girls.
B-Family history is commonly positive in Tics.
C-Tics disorders commonly presents with eye blinking or facial movements and occasional throat-clearing noises.
D-Transient tics of childhood persist from weeks to less than a year and generally do not require drug therapy.
E-Chronic motor tic disorder characteristically involves up to three muscle groups simultaneously and may occur throughout life.
F-Non of the above.
5-Which of the following statements is true:
A-Gilles de la Tourette syndrome can be inherited as autosomal dominant disorder.
B- Gilles de la Tourette syndrome is characterized by motor and vocal tics, and compulsive behaviors including touching, licking.
C-Gilles de la Tourette syndrome is a lifelong condition, and the prognosis generally depends on the severity of the symptoms during adolescence.
D-All of the above.
E-Non of the above.
A child who is studying at first grade intermediate school was referred from endocrinologist as a case of depression with main complains of refusing to go to school anymore. The child is known to have insulin depended diabetes mellitus and has just recently received the diagnosis of celiac disease. The child looked depressed and had feeling of hopelessness and his tears was running rather easily. The most likely diagnosis in this case:
A-Adjustment disorder.
B-Major depressive illness.
C-Situational depression.
D-School phobia.
E-A and C.
F-Non of the above.
A ten-year old boy was frequently saying Shut up when his mother talks with him and was also beating his younger sister when become angry for minor reasons. At school he was frequently fighting with other students. While waiting his turn, he also fought with an other child.
1-The boy may have one of the following disorders except:
A-Aggressive psychopathy.
B-Oppositional defiant disorder.
C-Tourette syndrome.
D-Conduct disorder.
E-A and C.
2-Children with Oppositional defiant disorder do all of the followings except:
A-They argue with adults, and lose temper and become angry frequently.
B-They annoy others deliberately.
C-Blames others for their mistakes and problems.
D-Violates basic rights of others.
E-Non of the above.
3-Which of the following statements is true about conduct disorders:
A-Children with conduct disorder are aggressive and fight with other children frequently.
B-They violate social norms and may call name their parents.
C-May destroys property.
D-May become aggressive against animals and harms them.
E-Childhood conduct disorder may be precursor of anti-social personality disorder which is associated with law breaking and is diagnosed after the age of eighteen years.
F-All of the above.
A girl at fourth grade primary school who was previously normal and doing well at school until two days ago. The teacher punished her by standing alone for 10 minutes near the blackboard in the class. At about 7 pm, the parents noticed that the girl was frequently blinking her eyes. The girl is most likely has:
A-Rheumatic chorea.
B-Tourette syndrome.
C-Huntigton disease.
D-Motor tic disorder.
E-All of the above.
F-Non of the above
A girl who was doing well at first grade intermediate school was referred from the dermatology clinic at Baghdad Teaching Hospital to our pediatric psychiatry clinic despite that the parents took her to the dermatologist because of hair loss (Figure-1). The dermatologist must have suspected:
A-A disorder that is related to the family of obsessive compulsive disorders.
B-Body focused repetitive disorders.
C-Trichotillomania.
E-All of the above.
F-Non of the above.
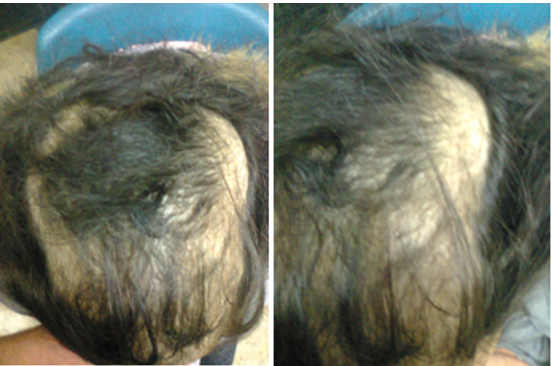
Figure-1
Answers:Case-1 | ||||
1-E | 2-E | 3-E | 4-F | 5-F |
6-F | 7-D | 8-B | 9-F | 10-E |
Answers: Case-2 | ||||
1-A | 2-E | 3-F | 4-A | 5-F |
6-C | 7-E | 8-E | 9-E | 10- |
Answers: Case-3 | ||||
1-D | ||||
Answers: Case-4 | ||||
1-F | 2-F | 3-E | 4-D | 5- |
Answers: Case-5 | ||||
1-E | 2-C | 3-E | 4-D | 5-E |
Answers: Case-6 | ||||
1-E | 2-A | 3-F | 4-E | 5-E |
Answers: Case-7 | ||||
1-A | 2-D | 3-F | 4-E | 5- |
Answers: Case-8 | ||||
1- E | 2-F | 3- | 4- | 5- |
Answers: Case-9 | ||||
1-E | 2-C | 3-C | 4-A | 5-D |
Answers: Case-10 | ||||
1-E | ||||
Answers: Case-11 | ||||
1-D | 2-D | 3-F | 4- | 5- |
Answers: Case-12 | ||||
D | ||||
Answers: Case-13 | ||||
E | ||||
The author would like to express his gratitude for the parents of the children who willingly accepted publishing the photos of their children.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
